Appendix 4.O – Integrated Prevention Management: A Way Forward?
Occupational health and safety stakeholders, who are responsible for the prevention of injuries and health problems, and return-to-work stakeholders, who are responsible for the prevention of long-term disability, have different roles and responsibilities. They are not always part of the same structures within organizations. They are therefore often called upon to play different roles (prevention representative, health and safety committee members, union representatives, supervisors, physicians, health care workers, insurer workers). Although this is not always the case, each actor is involved for a specific mandate. This can make communication and coordination with actors involved at other levels of prevention difficult and leads to undesirable effects.
The following sections discuss three levels of prevention, possible causes of difficulties in coordinating prevention efforts in organizations, and a relatively new concept, “integrated prevention”. Although research has yet to evaluate its effects, the following concepts will help you better understand its potential.
The three levels of prevention
The following is the definition of the three levels of prevention from the perspective of workplace actions, along with a table (Table N.1) highlighting who is affected, what effects are targeted, and what actions should be taken at each level. This is an adaptation of information contained in IWH (2015) and Vézina, Calvet, & Roquelaure (2018).
Primary prevention aims to prevent the development of health problems or accidents in workers. This is accomplished by:
- prevent or reduce exposure to hazards leading to health problems or injuries, if possible, as soon as new work situations arise
- change risky behaviors;
- increase resistance to health problems or injuries when exposed.
Secondary prevention aims to reduce the impact of an injury or health problem that has already occurred. This is accomplished by:
- detect and treat the problem as early as possible (e.g., when the first symptoms appear) to stop or slow its progression;
- encourage personal strategies for relapse prevention;
- prevent long-term problems by implementing programs to restore original health and function.
Tertiary prevention aims to mitigate the impact of a health problem or injury that is likely to be prolonged over time. It includes actions aimed at promoting the return to work (RTW) of workers following sickness absence.
This requires helping workers manage their often complex health problems and injuries (e.g., chronic illnesses, permanent impairments) over the long term to improve their ability to function and their quality of life.
The content of this website focuses on tertiary prevention.
Table N.1 ─ People involved, intended effects, and actions to be taken at each prevention level.
| Levels of prevention | People involved | Intended effects | Actions to be taken |
|---|---|---|---|
|
Primary |
Population potentially at risk but not yet affected by the targeted health problem |
To reduce the incidence of a disease in a population, thus reducing the risk of new cases. |
Individual (personal hygiene, diet, physical activity, vaccination, etc.) and collective (drinking water supply, waste disposal, food safety, workplace hygiene, etc.) prevention measures. |
|
Secondary |
Population affected by the targeted health problem. |
Decrease the prevalence of a disease in a population, thus reducing the duration of the disease. |
Actions such as early detection and treatment of early disease. |
|
Tertiary |
Population that has experienced the targeted health problem and be left with after-effects |
Reduce the prevalence of chronic disabilities or recurrences and minimize functional disabilities resulting from the disease. Promote professional and social reintegration |
All actions that achieve the intended effects. This extends prevention to the field of rehabilitation. |
Issues of communication and coordination of prevention efforts in organizations
Communication and coordination of efforts between the three levels of prevention are challenging. The situations created by ineffective communication and coordination between actors can be of different kinds. Some examples include:
- The occurrence of the same occupational injuries, failing to intervene by taking advantage of the organization’s occupational injury indicators.
- Assigning a worker to a position that has no productive value in order to reduce the amount of time he or she is absent without disrupting the production line. This type of assignment can lead to a decrease in the worker’s motivation as well as the judgment of colleagues.
- When the company is unionized, late union involvement in the RTW process.
- Non-involvement of the worker or immediate supervisor in the design of the RTW plan leading to unchanged RTW conditions and relapse of the worker.
- Underutilization of specialized external professional resources when needed.
Vézina et al. (2018) associate several causes for these problems. Interventions are often piecemeal depending on the requesters (insurer, employer, union, health workers), their vision or their investment logic. Several actors or sectors involved, from various disciplines and with responsibilities that respect different logics (prevention models), thus pave the way for practices that can be detrimental to each other. Actors, intervening at a micro level of the organization, can harm each other through a lack of overview. Yet, some actions have the potential to serve to achieve the intended effects of multiple levels of prevention at once (Memish, Martin, Bartlett, Dawkins, & Sanderson, 2017).
In large companies such as the hospital settings studied by Yassi, Ostry, and Spiegel (2014), managers belong to different teams. Therefore, communication does not always occur between these teams. Indeed, responsibility falls to different parts of the organization: returns to work are managed by human resources, risk factor reduction by health and safety managers, and new accommodations by production managers. But who is responsible for job retention once the return to work is successful?
In smaller companies, one might think that the difficulties of communication and coordination of actions are reduced, since the same actors are involved in prevention and rehabilitation. However, there is no evidence to support this and little knowledge or models to provide insight in these settings.
The context of large companies makes it difficult to ensure the cohesion of actions carried out in primary, secondary and tertiary prevention. The context of small businesses is little described in the literature. This highlights the need for applicable operating models for workplaces.
Integrated prevention or better yet, integrated prevention management.
Integrated prevention aims at the design or transformation of work situations through coordinated prevention actions carried out by the actors of the work environment (macro level of the company). It implies the integrated management of prevention actions (primary, secondary, tertiary) carried out by the actors of a work environment (organization or company). This global approach involves:
- to prevent the onset of the first physical or psychological symptoms of all workers;
- to avoid the transition to chronicity for some of these workers;
- to promote the return and retention of those who have been absent from work due to severe chronic MSD or CMD conditions.
This approach requires a shift from diagnosis of work situations to diagnosis of the company in terms of prevention management. This means that interventions in tertiary prevention can make it possible to move from an individual level to a collective level, in order to keep a group of workers at work in the long term. To do this, communication must be established between the actors in the organization responsible for RTW, working mainly on tertiary prevention, and those involved in the OHS committees (primary and secondary prevention). Refer to Figure 1.N (Calvet et al., 2015) to understand how integrated prevention management works.
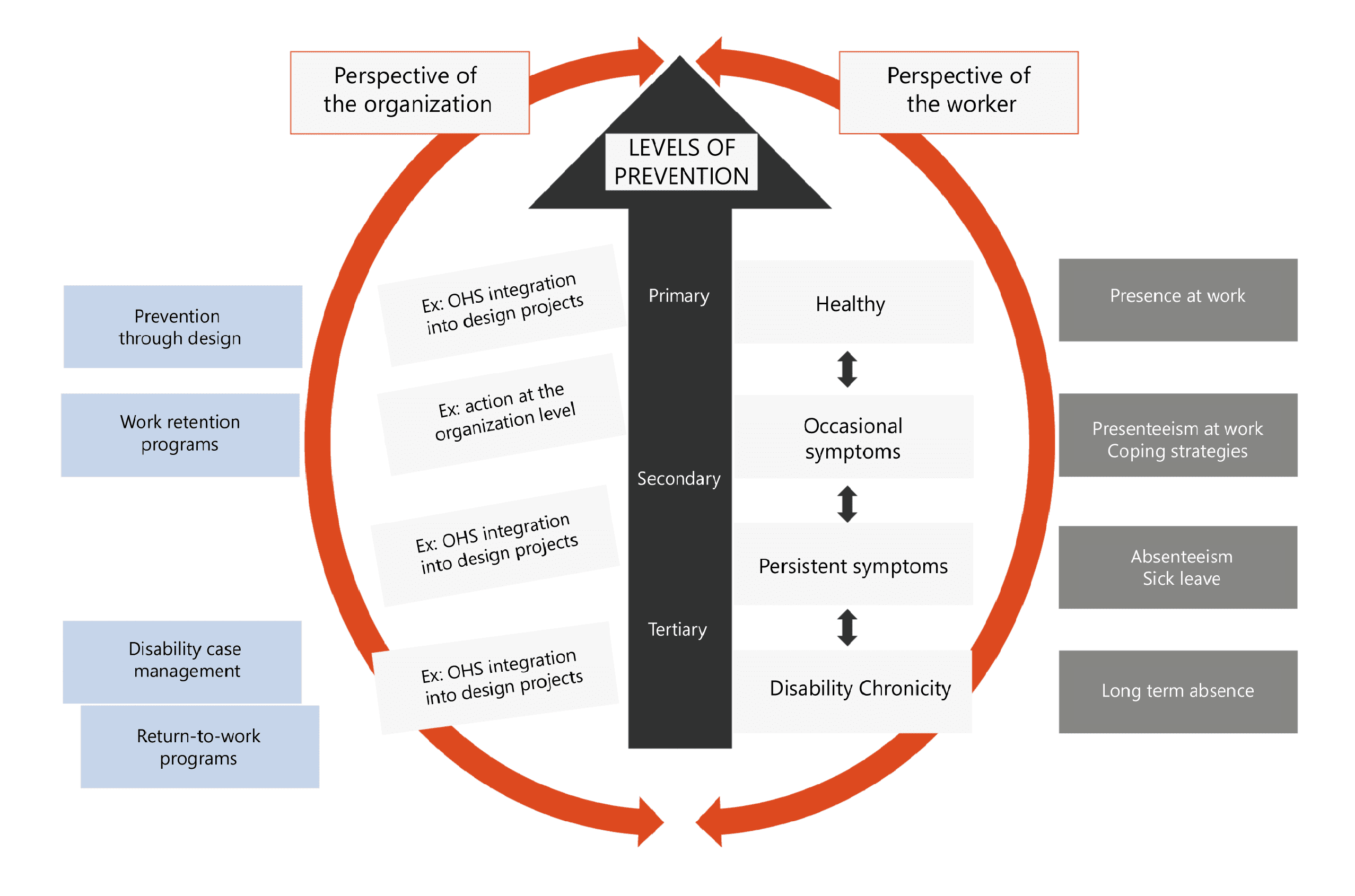
Figure N.1 (adapted from Calvet et al., 2015). Illustration of the relationships between the concepts involved in integrated prevention management. Note first the workplace perspective (left) and the individual perspective (right). The type of action to be taken at each level of prevention applies to workers with different health (symptom intensity and duration) and disability status. The blue arrow pointing upwards implies that actions carried out in tertiary prevention (e.g. by human resources) should be considered in secondary prevention and, even better, in primary prevention (e.g. by OHS committees).
Examples from around the world
Integrated prevention management has not been scientifically evaluated for its effectiveness or cost-effectiveness, as it is currently not widely used in companies. A systematic literature review (Memish et al., 2017) identified 20 practice guides on managing mental health in the workplace from different countries or organizations (Australia, Canada, Ireland, WHO, United Kingdom, United States, European Union). The guidelines were evaluated using seven criteria, with a score of 100% indicating the presence of primary, secondary and tertiary prevention recommendations, as well as recommendations designed to target both individual (worker) and organizational factors. The guides’ scores ranged from 21% to 100%. Only one guide achieved a score of 100% (Canadian Mental Health Commission, 2013, confirmed in 2018). This guide is based on the available evidence (LaMontagne et al., 2014).
References:
Calvet, B., Vézina, N., Nastasia, I., Laberge, M., Rubiano, P., Sutan-Taïeb, H., . . . Durand, M.-J. (2015). La prévention intégrée : analyse du concept pour une meilleure pratique. Communication présentée au 83e congrès de l’Association francophone pour le savoir : L’incapacité au travail au Québec : où en sommes-nous? Recherches, implantation et défis, Rimouski, 25-29 mai
Calvet, B., Vezina, N., Laberge, M., Nastasia, I., Sultan-Taieb, H., Toulouse, …Durand, M.J., 2021. Integrative prevention and coordinated action toward primary, secondary and tertiary prevention in workplaces: A scoping review. Work, (70), 893-908. doi : 10.3233/WOR-213609
Institute for Work & Health. (2015). What researchers mean by primary, secondary and tertiairy prevention. Atwork, (80), 2.
LaMontagne, A. D., Martin, A., Page, K. M., Reavley, N. J., Noblet, A. J., Milner, A. J., . . . Smith, P. M. (2014). Workplace mental health: Developing an integrated intervention approach. BMC Psychiatry, 14. doi: 10.1186/1471-244X-14-131
Memish, K., Martin, A., Bartlett, L., Dawkins, S. et Sanderson, K. (2017). Workplace mental health: An international review of guidelines. Preventive Medicine, 101, 213-222. doi: 10.1016/j.ypmed.2017.03.017
Vézina, N., Calvet, B. et Roquelaure, Y. (2018). Vers des programmes de gestion intégrée de la prévention aux niveaux primaire, secondaire et tertiaire. Dans M.-J. Durand et É. Vaillancourt (Édit.), Incapacité au travail au Québec : éléments de réflexion et d’intervention quant aux nouveaux défis (p. 11-31). Longueuil, QC: CAPRIT.
Yassi, A., Ostry, A. et Spiegel, J. (2014). Injury prevention and return to work: Breaking down the solitudes. Dans J. Frank et T. Sullivan (Édit.), Preventing and managing disabling injury at work (p. 93-104). Boca Raton, FL: CRC Press.
Groupe CSA. (2018). Santé et sécurité psychologiques en milieu de travail : prévention, promotion et lignes directrices pour une mise en œuvre par étapes. Norme CAN/CSA-Z1003-13/BNQ 9700-803/2013 (C2018). Mississauga, ON: Groupe CSA. From https://store.csagroup.org/ccrz__productdetails?viewstate=detailview&cartid=&sku=can/csa-z1003-13/bnq%209700-803/2013&iscsrflow=true&portaluser=&store=&cclcl=fr_CA
CSA Group. (2018). Psychological health and safety in the workplace: Prevention, promotion, and guidance to staged implementation. Norme CAN/CSA-Z1003-13/BNQ 9700-803/2013 (C2018). Mississauga, ON: CSA Group. From https://store.csagroup.org/ccrz__productdetails?viewstate=detailview&cartid=&sku=can/csa-z1003-13/bnq%209700-803/2013&iscsrflow=true&portaluser=&store=&cclcl=fr